If you searched for a clinical depression test or a depression test doctors use, the most useful answer is this: doctors often use screeners such as the PHQ-9 depression test, but a diagnosis of clinical depression is not made from one quiz alone. A clinician looks at symptom patterns, duration, daily impairment, safety risk, medical causes, medications, substances, grief, trauma, and possible bipolar symptoms before deciding whether major depressive disorder or another condition fits.
Quick answer
A screening score can tell you whether depression symptoms are worth discussing. A diagnosis requires a clinical interview and context. Use an online screener as a starting point, then bring the score and symptom examples to a qualified healthcare professional.
Table of contents
Screening Test vs Clinical Diagnosis
A depression screening test asks structured questions and returns a score. That score estimates symptom severity during a defined time window, often the past two weeks. Screening is useful because it makes vague distress easier to describe. It can also help track whether symptoms are improving or getting worse over time.
A clinical diagnosis is broader. A clinician asks whether symptoms meet a recognizable pattern, how long they have lasted, whether they interfere with life, whether there are safety concerns, and whether another explanation is more likely. For major depressive disorder, depressed mood or loss of interest is especially important, along with other symptoms such as sleep change, appetite or weight change, low energy, guilt or worthlessness, concentration problems, psychomotor changes, and thoughts of death or self-harm.
| Question | Screening test | Clinical diagnosis |
|---|---|---|
| What it does | Estimates symptom severity | Determines whether a disorder fits the full picture |
| Who can complete it | You can usually complete it yourself | A qualified clinician makes the diagnosis |
| Output | Score range or risk category | Clinical impression, diagnosis, and treatment plan |
| Main limitation | Cannot rule out other causes | Requires time, history, and professional judgment |
What Depression Tests Do Doctors Commonly Use?
Different settings use different tools, but the PHQ-9 is one of the most common depression screeners in primary care and behavioral health. It is short, scored from 0 to 27, and asks about symptom frequency over the previous two weeks. A clinician may use it at the first visit and repeat it later to monitor change.
PHQ-9
The PHQ-9 is practical because it maps closely to common depressive symptom domains and includes a self-harm/death item that should never be ignored. A higher score can support the need for further evaluation, but it does not prove depression by itself. For example, poor sleep, appetite change, and fatigue may also come from medical illness, medication side effects, shift work, chronic pain, or substance use.
PHQ-2 and follow-up screening
Some clinicians start with the PHQ-2, a two-question screen about low mood and loss of interest. If it is positive, they may follow with the PHQ-9 or a fuller interview. This approach saves time in busy primary care settings while still catching people who need more support.
Other questionnaires
Some mental health professionals use additional scales such as the Beck Depression Inventory, Hamilton Depression Rating Scale, Montgomery-Asberg Depression Rating Scale, or specialized questionnaires for postpartum depression, adolescents, anxiety, trauma, or substance use. The best tool depends on the person's age, situation, setting, and reason for evaluation.
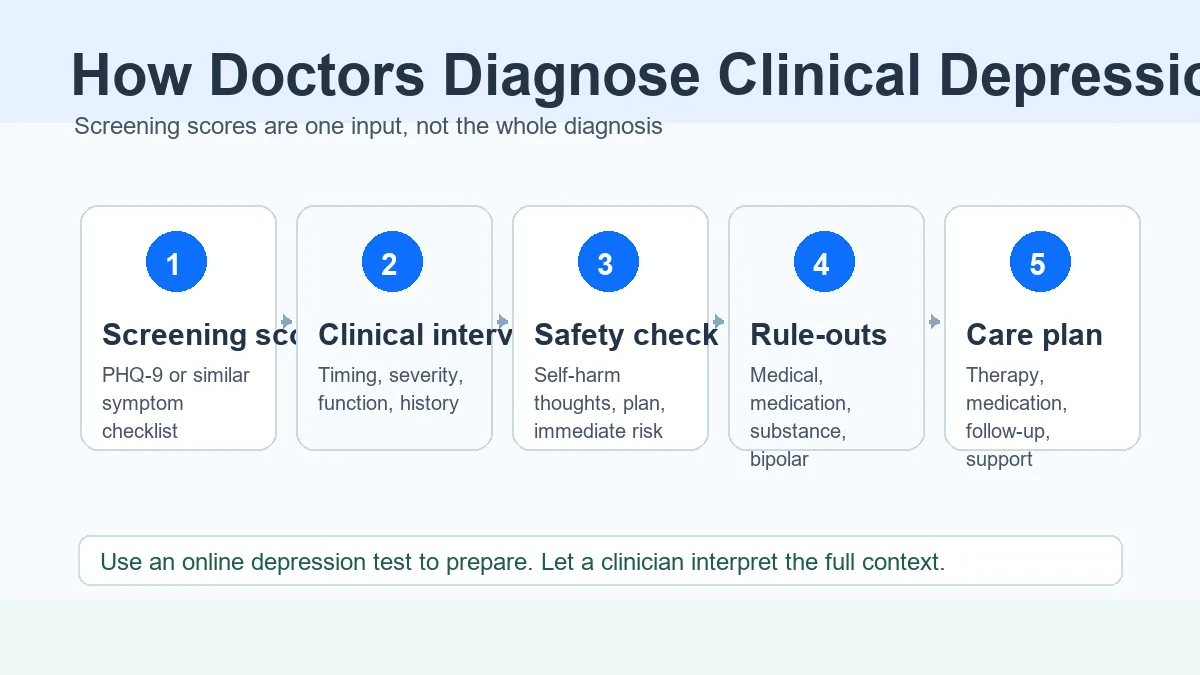
How Doctors Diagnose Clinical Depression: The Usual Steps
The exact process varies, but most evaluations follow a similar logic. The clinician is trying to answer two questions at the same time: "Do the symptoms fit depression?" and "Is there anything urgent or different that changes the plan?"
1. Symptom timing and pattern
Expect questions about when symptoms started, how often they occur, whether they last most of the day, and whether the pattern has persisted for at least two weeks. The clinician also asks about previous episodes and whether symptoms are new, recurrent, or chronic.
2. Functional impact
Depression is not only about feeling sad. Clinicians ask how symptoms affect work, school, parenting, relationships, hygiene, sleep, eating, concentration, motivation, and responsibilities. Impairment helps distinguish a passing rough period from a clinical concern.
3. Safety assessment
Any thoughts of death, self-harm, or suicide require direct follow-up. A clinician may ask about plans, intent, access to means, previous attempts, protective factors, and whether immediate support is needed. This is a standard safety step, not a judgment.
4. Mental health history
The evaluation often covers anxiety, panic, trauma, obsessive symptoms, eating concerns, substance use, attention problems, psychosis symptoms, and past treatment. This helps avoid treating one symptom while missing the larger pattern.
5. Treatment discussion
If depression is likely, the next step may include therapy, medication discussion, lifestyle supports, follow-up screening, crisis planning, sleep and substance changes, or referral to a specialist. Treatment depends on severity, preference, history, access, and safety.
What Clinicians Need to Rule Out
Many depression symptoms overlap with other conditions. A careful evaluation protects you from a too-simple answer. This is especially important if symptoms started suddenly, changed after a medication, came with new physical symptoms, or include periods of unusually elevated mood.
Bipolar symptoms
Clinicians usually ask about past periods of unusually high energy, decreased need for sleep, racing thoughts, impulsive behavior, risky decisions, or feeling unusually powerful or irritable. These symptoms can change treatment decisions, so they matter even if the current problem feels like depression.
Medical and medication causes
Depending on the situation, a doctor may review thyroid disease, anemia, vitamin deficiencies, chronic pain, sleep apnea, pregnancy or postpartum changes, neurological conditions, alcohol or drug use, and medication side effects. Lab testing is not a depression test, but it can help identify medical contributors.
Grief, trauma, burnout, and stress
Stressful life events can cause symptoms that look similar to depression. That does not mean the distress is less real. It means the clinician needs to understand context: what happened, how long symptoms have persisted, whether there is trauma, and whether the response has become impairing or dangerous.
Do not use a score as the whole story
A PHQ-9 score can be very helpful, but the same score may mean different things in two people. Bring examples, timing, medications, health changes, and safety concerns so the clinician can interpret the score correctly.
What to Bring to a Depression Evaluation
You do not need perfect notes, but a little preparation can make the visit more useful. If you are nervous, write short bullet points in advance and hand them to the clinician.
- Your PHQ-9 score or another recent screening result.
- When symptoms started and whether they happen daily, most days, or in waves.
- Examples of how mood, sleep, appetite, energy, focus, and motivation have changed.
- Any self-harm thoughts, even if you do not intend to act on them.
- Current medications, supplements, alcohol or drug use, and major health changes.
- Past episodes of depression, anxiety, trauma, mania-like symptoms, or treatment.
- What you want help with first: sleep, work function, safety, therapy, medication, or diagnosis clarity.
For symptom language, our SIGECAPS guide can help you organize what you are experiencing. If you already have a score, read the results interpretation guide to understand what the range may suggest before your appointment.
If you might not be safe
Do not wait for a routine appointment. In the United States, call or text 988. If there is immediate danger, call emergency services or go to the nearest emergency department.
FAQ About Clinical Depression Tests
Can an online clinical depression test diagnose me?
No. It can help identify symptoms and estimate severity, but diagnosis requires a clinical evaluation. Online screeners are best used as preparation for a conversation with a healthcare professional.
What test do doctors use for depression?
Many doctors use PHQ-9 because it is short, scored, and easy to repeat. Some clinicians use other scales depending on the setting and the person's needs.
Does a high PHQ-9 score always mean major depressive disorder?
Not always. A high score means symptoms are significant and deserve attention. A clinician still needs to consider medical causes, medication effects, substances, bipolar symptoms, grief, trauma, and other mental health conditions.
Can depression be diagnosed without lab tests?
Yes. Depression is diagnosed clinically through symptoms, duration, impairment, and context. Lab tests may be used to check for medical contributors, but there is no routine blood test that by itself diagnoses depression.
Should I take a depression test before seeing a doctor?
It can help. A recent PHQ-9 score gives the clinician a structured snapshot. Still, share your examples and concerns, not just the number.
Related resources
Take the PHQ-9 Depression Test
Use a scored screener before a clinical conversation.
Results Interpretation
Understand PHQ-9 score ranges and next steps.
SIGECAPS Depression Mnemonic
Organize symptoms before an appointment.
Free Depression Screening Tools
Compare screeners and when each tool fits.
References and further reading
- National Institute of Mental Health: Depression
- American Psychological Association: Clinical practice guideline for depression
- NCBI Bookshelf: DSM-5 major depressive episode symptom criteria table
- American Psychological Association: PHQ-9 questionnaire and scoring reference
- Kroenke K, Spitzer RL, Williams JBW. The PHQ-9: validity of a brief depression severity measure. Journal of General Internal Medicine. 2001.